

Name has been changed to protect patient privacy. Clinical details, lab reports and messages are shared with the family’s explicit consent.
When Lalitha first came to us, she was not looking for dramatic weight loss. She was not chasing a number on the scale.
She had one quiet wish: to be strong enough to look after her daughter-in-law through the delivery of her first grandchild.
Her daughter-in-law had been through our sister brand Fertilia’s program and had conceived naturally after months of trying. Lalitha had watched that journey closely. And now, with a grandchild on the way, she was worried about something very practical. Could she stand for long hours in the kitchen? Could she pick up a baby without wincing? Could she be the support her daughter-in-law would need in those exhausting first weeks?
At 60, postmenopausal, living with rheumatoid arthritis and cholesterol that had been creeping up for years, she genuinely did not know.
This is the story of what happened over the next 3 months.
Where It Started
Lalitha had been managing rheumatoid arthritis for several years, under the care of an arthritis specialist. Over time, her condition had progressed to the point where routine activities like walking, standing, and even lifting her hands had become difficult.
Her daily habits told a story too. Her mornings typically started with sugared coffee, biscuits, and fruit on an empty stomach. By evening, she was exhausted. Her meals leaned heavily on carbohydrates. Sugar cravings were persistent. And her joints, unsurprisingly, were getting worse.
When she enrolled with us on October 1st, her baseline report was as follows:
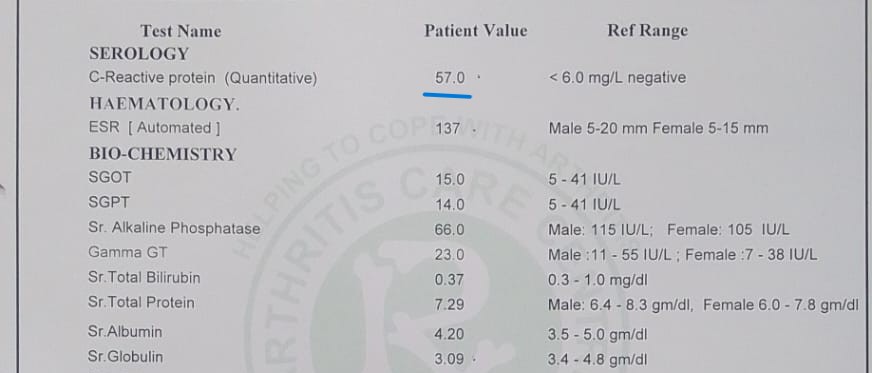
Her baseline serology. C-Reactive Protein was 57 mg/L, more than nine times the upper limit of normal. ESR was 137, another marker of active inflammation.
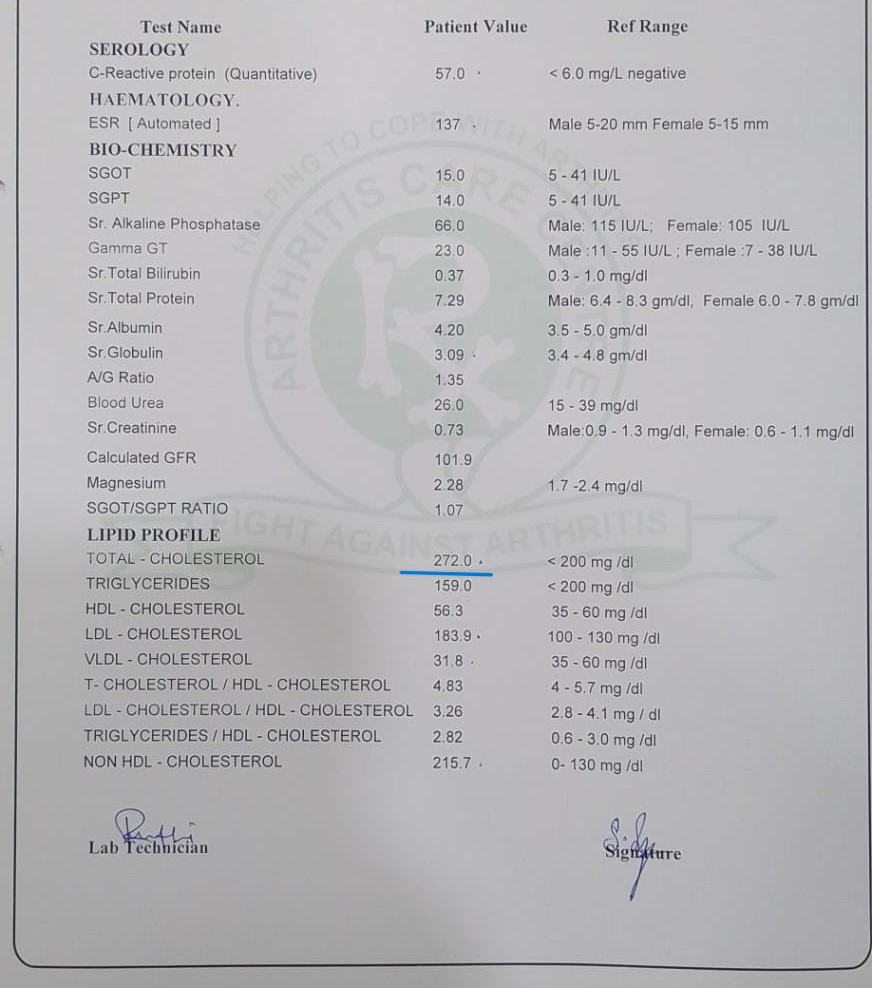
Her baseline lipid profile. Total cholesterol: 272 mg/dL. LDL: 183.9 mg/dL. Non-HDL cholesterol: 215.7 mg/dL. All elevated.
Her daughter-in-law later shared a line that has stayed with me:
“Mom’s CRP was never in normal level for years.”
That was the context we were working with. Years of persistent inflammation. Not a new flare. Not a temporary spike.
Why This Combination Matters After Menopause
Before we get to what we did, it helps to understand why rheumatoid arthritis + elevated cholesterol + postmenopause is a combination that deserves careful attention together, not in silos.
Oestrogen is quietly anti-inflammatory. When it declines at menopause, many women find that joint pain, stiffness, and body aches intensify even without an autoimmune condition. For a woman already living with rheumatoid arthritis, the loss of oestrogen’s protective effect can make symptoms more pronounced.
The same hormonal shift also affects how the body handles fats. Cholesterol and LDL typically rise after menopause, and the cardiovascular risk profile changes in ways that do not always show up on a regular health check.
Put together, a postmenopausal woman with RA is dealing with two systems that both need support: an inflammatory system that has lost a protective signal, and a metabolic system that is recalibrating. Treating either one in isolation often means the other keeps drifting.
This is the quiet reason so many women in Lalitha’s situation feel they are “on their way down” in their 60s. The biology is working against them on multiple fronts, and generic advice like “walk more” or “eat less oily food” is rarely specific enough to move the needle.
What We Did Not Do
Before I explain the plan, it is worth stating what we deliberately avoided.
We did not ask her to stop any of her arthritis medications. Those are prescribed by her specialist for a reason, and our role is to work alongside that medical care, not in place of it. Her rheumatologist continued to guide the medical side throughout.
We did not put her on an intense exercise regimen. Aggressive cardio and heavy training are often counterproductive for someone with active joint inflammation. They can increase damage, not reduce it.
We did not put her on an aggressive calorie restriction. At 60, with active inflammation and low energy tolerance, aggressive restriction triggers more fatigue, more cortisol, more muscle loss. It is exactly the wrong tool.
We did not give her a generic “anti-inflammatory diet” handout. She had seen enough of those. What she told us, through her daughter-in-law, was telling:
“A lot of doctors we see outside simply tell us to avoid carbs and balance our plates. But we were clueless what all that meant, and how we should do it for someone who is around 60.”
That gap, between well-intentioned advice and a plan a 60-year-old woman can actually follow on a Tuesday afternoon, was what we set out to close.
The Plan
Lalitha’s program was built around five specific interventions, each designed for her age, her joint condition, and her energy levels:
1. Targeted supplement support to address her nutrient deficiencies, support inflammation control, and protect joint health. This was personalised to her, not a generic stack.
2. A balanced, condition-specific diet without severe restriction. Normal, sustainable portions. The goal was not deprivation. It was consistency.
3. Strategic meal timing to reduce fatigue. Her old pattern of sugared coffee and biscuits on an empty stomach was quietly draining her all day. Spacing meals properly changed how her body regulated energy.
4. Simple strengthening exercises, customised to her joint tolerance and pain levels. Nothing dramatic. Just what her body could sustain.
5. Gentle walking, introduced progressively. We started where she was, not where a fitness chart said she should be.
Her daughter-in-law summarised the change in habit beautifully:
“Within a week of following proper balanced diet, she herself started seeing the difference and felt a lot better.”
The Diwali Story
One moment from the first month stands out, and it tells you everything about the philosophy of this program.
Diwali came two weeks into Lalitha’s plan. In South Indian homes, Diwali fasting is a serious affair, with strict food rules and long hours of physical activity around pooja preparations. Her daughter-in-law was worried. Would fasting derail the plan? Would her MIL end the day exhausted and in pain, as in previous years?
She reached out to Manisha, our nutritionist, who is also overseeing Lalitha’s day-to-day plan. Manisha designed fasting-compatible recipes based on what Lalitha could eat and avoid, food that was easy to make on pooja days, respected the spirit of the fast, and kept her steady through the long hours.
Her daughter-in-law’s message afterwards said:
“When she finished her fasting by evening she was still in good energy and no exhaustion despite heavy pooja work. We can’t thank the team enough.”
This is the difference between “be on a diet” and “have a plan that bends with your life.” Lalitha did not have to choose between tradition and her health. Both were accommodated.
The First Month
Within the first week, Lalitha noticed:
- Reduced knee stiffness in the mornings
- More stable energy through the day
- Better tolerance to daily movement
By three weeks in, she had her first follow-up bloods done. Her lipid profile had already started moving in the right direction, which surprised even her. When the results came in, her daughter-in-law wrote to me directly, and my reply was genuinely from the heart:
“This is great news. It is her consistency and trust.” That is what I wrote back, and I meant it. The plan matters, but consistency is what makes the plan work.
The 3-Month Results
By the end of 3 months, the numbers told a story that even I did not expect to see this cleanly.
Inflammation: CRP fell by 91%

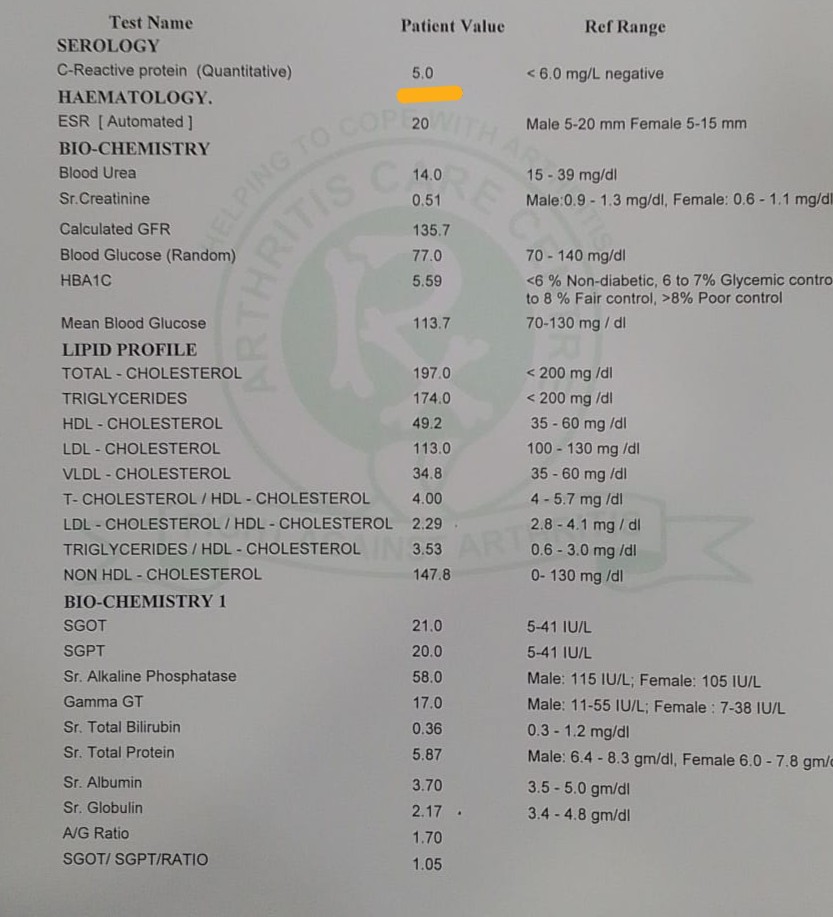
CRP: 57 → 5 mg/L (reference <6). A marker of inflammation that had been elevated for years is now within normal range.
Cholesterol: back in range

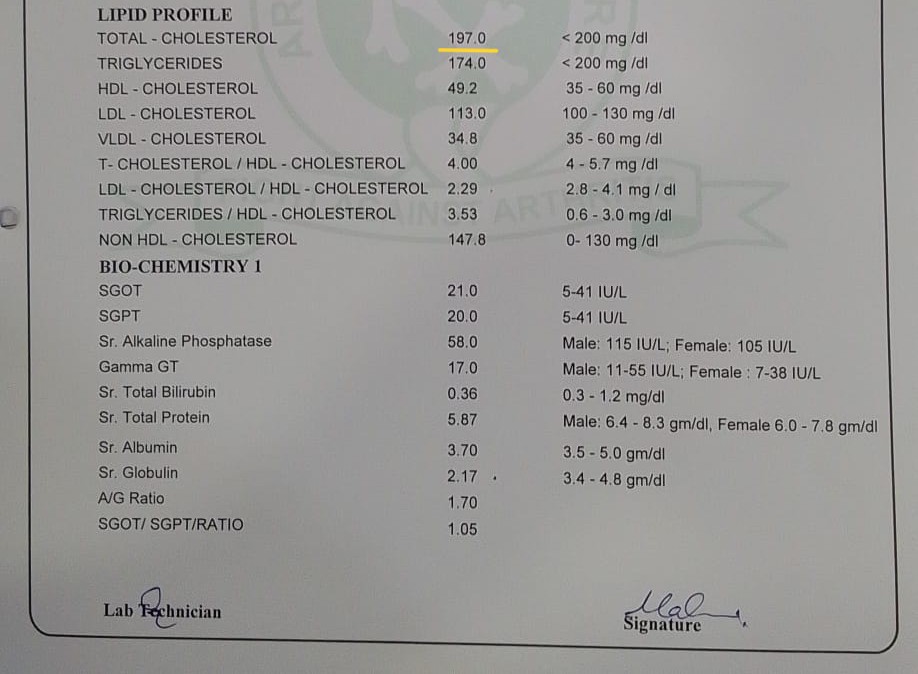
Total cholesterol: 272 → 197 mg/dL (reference <200). The lipid profile moved into normal range in under 20 days of starting the plan, and has held steady since.
LDL: from “high risk” to optimal

LDL cholesterol: 183.9 → 113 mg/dL (reference 100-130). Moved from the “high risk” band into the optimal range.
Weight: 6.3 kg lost safely

![]()
Weight: 77 → 70.7 kg. Lost gradually, without aggressive restriction or intense exercise. This pace matters: rapid weight loss in a 60-year-old with an inflammatory condition is rarely safe. Gradual loss protected her muscle, her joints, and her energy.
And the parts numbers cannot capture
- Knee stiffness reduced markedly. She could stand and walk without the pain she had grown used to.
- Fatigue improved. She no longer felt wiped out by early afternoon.
- Mobility returned. She could lift her hands, reach into overhead shelves, carry small loads. Small things, but not small at 60.
- Confidence came back. And with it, the feeling of being useful to her family again.
In Her Family’s Own Words
The longest message came from Lalitha’s daughter-in-law a few weeks before her delivery. With her family’s permission, here it is, in full context:
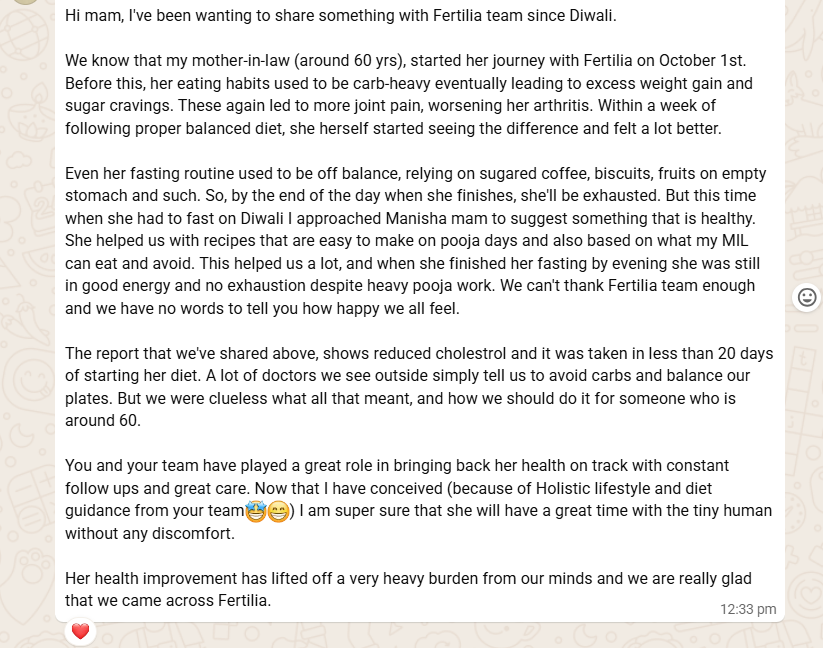
The parts that I keep returning to:
“Her health improvement has lifted off a very heavy burden from our minds.”
“Now that I have conceived, I am super sure that she will have a great time with the tiny human without any discomfort.”
“Her eating habits used to be carb-heavy eventually leading to excess weight gain and sugar cravings. These again led to more joint pain, worsening her arthritis. Within a week of following proper balanced diet, she herself started seeing the difference and felt a lot better.”
The reference to Fertilia in that message is intentional. Menolia is the perimenopause and menopause arm of my practice; Fertilia is the fertility arm. The same clinical team supports both, which is why a family often finds one brand first and then realises the support extends across generations.
What Lalitha’s Story Tells Us
I want to be careful about how I share this story. Every woman’s body is different. Not every 60-year-old with rheumatoid arthritis will see a CRP drop from 57 to 5. Some will have different medications, different disease activity, different starting points. That is real, and it matters.
But Lalitha’s story does tell us three things that I believe are true for most women in her situation:
1. Chronic inflammation responds to structured nutrition, even in your 60s. The body does not stop being responsive at a certain age. It just needs inputs it can actually use. Targeted, sustained changes can move markers that have been elevated for years.
2. Age-appropriate is safer AND more effective. In older women with inflammatory conditions, gentle and consistent beats intense and dramatic every time. The temptation to “finally get serious” with a strict diet and heavy workouts is almost always counterproductive.
3. Chronic conditions are not the end of the conversation about lifestyle. They are the beginning of a more careful one. Your rheumatologist, your cardiologist, your gynaecologist all remain important. A structured lifestyle plan does not replace them. It gives their prescriptions a better body to work in.
And one last thing, not a principle but a personal observation. What Lalitha wanted, really, was not a number. It was to stand beside her daughter-in-law and hold her first grandchild without her knees buckling. That is what lifestyle medicine can give back to women in menopause. Not dramatic before-and-after photos. The small, specific capacities of daily life.
💜 Navigating menopause alongside a chronic condition? Menolia’s programs are built with age, joint health, and existing medical care in mind. Start a conversation on WhatsApp. No pressure, just guidance.
Frequently Asked Questions
Can rheumatoid arthritis inflammation really improve through nutrition and lifestyle?
Yes, meaningfully. Inflammation markers like CRP respond to sustained nutritional changes, weight reduction, and consistent movement. This does not replace disease-modifying RA medications, which your rheumatologist manages. Nutrition works alongside medical treatment to reduce the inflammatory load on your body. In Lalitha’s case, her CRP moved from 57 to 5 mg/L in 3 months on a structured plan, while she continued under her specialist’s medical care.
Is it safe to lose weight after 60 with arthritis?
Safe weight loss after 60 is absolutely possible, but the pace and method matter. Aggressive calorie restriction and intense exercise can worsen inflammation, accelerate muscle loss, and strain joints. Lalitha lost 6.3 kg over 3 months, which works out to about 0.5 kg per week. That gradual pace preserved her muscle, was manageable on her joints, and produced lasting results. Losing weight this way also tends to reduce inflammation rather than trigger it.
Why does cholesterol rise after menopause, even without dietary changes?
Oestrogen has a protective effect on lipid metabolism. When oestrogen declines at menopause, total cholesterol, LDL, and non-HDL cholesterol typically rise, even if your eating habits have not changed. This is why many women are surprised when their lipid numbers worsen after 50. We cover this in detail here. The good news: diet and lifestyle changes that target postmenopausal metabolism can bring these numbers back into range, as Lalitha’s results show.
Can older women with chronic conditions safely fast during festivals like Diwali?
With the right support, yes. The risk with fasting at 60+ is not fasting itself, it is the poor-quality foods often used to break or sustain a fast, and the absence of structured meal timing. When Lalitha fasted for Diwali, our nutritionist designed fasting-compatible recipes that respected her tradition, her joint condition, and her energy needs. She finished the day with stable energy rather than exhaustion. Read more on menopause and fasting here.
Do I need to stop my arthritis medications or my gynaecologist’s medications to follow this program?
No. Menolia works alongside your existing medical care, not in place of it. Your rheumatologist handles your RA treatment. Your gynaecologist handles menopause-related medical decisions. We add the lifestyle layer, nutrition, targeted supplementation, movement, sleep, that helps your body respond better to everything your other doctors are already doing. Lalitha continued her specialist-led care throughout her program with us.
How quickly can inflammation markers improve?
It depends on the starting level and the consistency of the plan. Some markers, like lipid profile, can improve within 2-3 weeks, as Lalitha’s cholesterol did. CRP tends to respond more gradually, as it reflects deeper systemic inflammation. In Lalitha’s case, CRP had been elevated for years, and normalised over 3 months of consistent effort. Every woman’s timeline will be different.
💜 If you are in your 50s or 60s, navigating menopause alongside chronic pain, rising cholesterol, or low energy, you are not alone, and you are not out of options. Message Dr. Suganya on WhatsApp. A short conversation is often where the next chapter starts.
Related Reading
- Menopause Joint Pain: Why It Happens After 40
- Menopause Cholesterol: Why Your Numbers Changed
- Menopause Body Aches: Why It Happens, What Helps
- Menopause Weight Gain: What Actually Works
- Menopause Supplements: An Evidence-Based Guide
- Menopause Bone Health & Osteoporosis: Indian Women
This is the first in our series of patient case studies on Menolia. Every story is real, verified, and shared with the patient’s and family’s explicit consent. Names and identifying details are changed to protect privacy.



